ACR Statement on JAMA CT Scan Radiation Study (Smith-Bindman, et al)
April 14, 2025
Read time: 3 min
The theoretical radiation risk proposed by Smith-Bindman, et al, is consistent with prior statistical modeling studies that are not based on actual patient outcomes. The National Council on Radiation Protection and Measurement has reported that even with increased CT use, advances in technology and imaging protocol optimization have reduced population radiation burden (medical radiation dose per capita/person). There are no published studies directly linking CT scans (even multiple CT scans) to cancer. Americans should not forgo necessary, life-saving medical imaging and continue to discuss the benefits and risks of these exams with their healthcare providers.
No medical test, including those utilizing ionizing radiation, should be performed unless the medical benefits gained from the test clearly outweigh any associated risk. Radiologyinfo.orgoffers easily understood information on imaging and radiation oncology procedures – including how these work, how to prepare for them, benefits and risks, and relative radiation dosesused.
Patients should keep a record of their (or their loved ones’) imaging procedures. Before undergoing any imaging study, particularly those that involve radiation exposure, patients should ask their physician or other medical provider the following questions:
How will having this exam improve my health care?
Are there alternatives that do not use radiation which are equally as good (e.g. MRI, ultrasound, etc.)?
Is this facility ACR Accredited (which ensures high quality standards, including regular surveys of the equipment by medical physicists, certified technologists performing the exams, and interpretation by radiologist physicians who meet stringent education and training standards)?
The American College of Radiology® (ACR®) has a long history of medical imaging dose optimization with quality and safety efforts that positively impact patient care.
The ACR co-founded the Image Gently® and Image Wisely® initiatives to help providers avoid ordering low value imaging and optimize radiation dose used in many scans. The ACR partnered with the American Board of Internal Medicine Foundation, Consumer Reports and others to launch the Choosing Wisely effort to identify exams whose necessity (and alternatives) should be discussed before ordering.
ACR will continue to work with decision makers, federal and state agencies, insurers and others to ensure Americans continue to have access to safe, high-quality radiologic care.
To speak with an ACR expert, contact Shawn Farley at PR@acr.org or 703-869-0292.
Cardiovascular ( CV) diseases are the leading cause of death among women, responsible for 35% of all female deaths globally, according to 2019 data. Alarmingly, myocardial infarction cases are rising among younger women. To address this, the Spanish Society of Cardiology’s (SEC’s) Working Group on Women and Cardiovascular Disease (SEC-GT CVD in Women) and the Association of Preventive Cardiology convened a multidisciplinary panel of experts from various Spanish societies and associations.
Representatives from gynaecology, endocrinology, paediatrics, primary care, family medicine, and midwifery collaborated to create a consensus document. This clinical guideline, approved by the SEC and published in the English edition of Revista Española de Cardiología, aims to assist healthcare professionals in diagnosing and managing women’s CV health, focusing on gender-specific differences.
Disease Prevention
Early detection of CV risk factors in women is critical. “This guide aims to raise awareness among healthcare professionals about the importance of preventing CVD in women, highlight the differences between men and women, and provide specific preventive recommendations tailored to the different stages of a woman’s life,” Dr Antonia Sambola, coordinator of SEC-GT CVD in Women and researcher at the Department of Cardiology, Vall d’Hebron University Hospital and Research Institute in Barcelona, Spain, told Univadis Spain, a Medscape Network platform.
However, Sambola stressed the importance of implementation: “A clinical guide that is not implemented is just paper. It is vital that this guide is implemented in clinical practice. For this reason, the SEC will undertake several initiatives to disseminate it, including meetings with representatives from the Ministry of Health to ensure it is distributed to the autonomous communities.”
Age-Specific Risks
The guidelines highlight age-specific CV risks for women.
In adolescent girls (10-21 years of age), key risk factors include a higher fat-to-lean mass ratio than that in boys (25% vs 14%), reduced physical activity, and higher smoking rates.
In women aged over 21 years, conditions such as polycystic ovary syndrome (PCOS), hypogonadotropic hypogonadism, and premature ovarian insufficiency (POI), all characterised by oestrogen deficiency, significantly increase CV risk. These hormonal imbalances are linked to metabolic disorders such as insulin resistance, central obesity, dyslipidaemia, and hypertension.
Menopause is associated with oestrogen production, leading to metabolic changes, including central abdominal fat accumulation, obesity, sarcopenia, and dyslipidaemia, which increase the risk for myocardial infarction and cerebrovascular events.
Hormone replacement therapy (HRT) is recommended for premenopausal women with POI or hypogonadotropic hypogonadism if there are no contraindications. Transdermal oestrogens have a more favourable impact on CV risk biomarkers than oral formulations.
Menopause is associated with reduced CV protection due to decreased oestrogen production. Metabolic changes during this phase, including central abdominal fat accumulation, obesity, sarcopenia, and dyslipidaemia, increase the risk for myocardial infarction and cerebrovascular events, particularly in cases of early menopause.
Recent studies have found HRT to be the most effective intervention for symptom relief and improved quality of life. These measures can reduce CVD risk and all-cause mortality in women aged under 60 years and within 10 years of menopause onset. However, HRT is not recommended for patients with high CV risk or pre-existing CVD.
Pregnancy Risks
Pregnancy causes significant CV changes, necessitating close monitoring. In women with pre-existing cardiometabolic risk factors or genetic or environmental predispositions, the physiological stress of pregnancy can lead to adverse outcomes, such as hypertensive disorders, intrauterine growth restriction, small-for-gestational-age neonates, placental abruption, preterm birth, and gestational diabetes mellitus (GDM). Women with a history of adverse pregnancy outcomes have a higher long-term risk for CVD.
Pre-pregnancy evaluations and early detection during weeks 11-13 of pregnancy are critical for identifying CV risks. Hypertensive disorders affect 10% of pregnant women, and GDM is another significant risk factor.
Additional Risks
Classic CV risk factors in women include smoking, obesity, hypertension, diabetes, and dyslipidaemia. Additional factors included:
Breast cancer survivors face higher risks for heart failure and myocardial ischaemia due to latent cardiac effects from cancer treatments.
Psychosocial stress: Strongly associated with the development and progression of CV atherosclerosis.
Autoimmune diseases: Conditions such as systemic lupus erythematosus and rheumatoid arthritis significantly increase the risk for CV disease.
Gender-Specific Challenges
“Being a woman is itself a risk factor for CVD,” explained Sambola. She highlighted three key issues: Inadequate medical training in gender-specific disease management, lack of routine screenings for women-specific CV risks, and widespread public misconceptions about CVD being less fatal than breast cancer.
Public awareness campaigns are essential to address these gaps. These should focus on age-specific CV self-care measures, such as quitting smoking and alcohol, engaging in physical activity, and routine health checks for glucose, blood pressure, and body weight.
“Finally, all women with early menopause, POI, and PCOS should undergo routine CV screenings,” concluded Sambola.
This story was translated from Univadis Spain using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
New Data Show Rise in Early-Onset CRC Extends Beyond High-Income Countries
Edited by Alexandra Graziano
February 28, 2025
TOPLINE:
The increase in incidence of early-onset colorectal cancer (CRC) is no longer confined to high-income nations. A recent study found that rates are also rising in Latin America, Asia, and Eastern Europe. Of the 50 countries analyzed through 2017, 27 showed a rising incidence of the disease among people younger than 50 years.
METHODOLOGY:
The primary objective was to examine CRC incidence trends in younger adults compared with older adults by analyzing data from 50 countries and territories including a dozen countries not previously explored, such as Argentina, Belarus, Chile, Ecuador, Kuwait, Qatar, Thailand, and Uganda.
The analysis included CRC incidence data from the World Health Organization–International Agency for Research on Cancer Incidence in the Five Continents Plus database, which covered 27 of the 50 countries and territories. Data from the remaining 23 were pulled from one or more subnational population-based cancer registries.
Researchers examined age-standardized incidence rates per 100,000 person-years for early-onset (aged 25-49 years) and late-onset (aged 50-74 years) CRC diagnosed between 1943-2003 and 2015-17.
TAKEAWAY:
The highest rates of early-onset CRC incidence were found in Australia (16.5 per 100,000 person-years), Puerto Rico (15.2 per 100,000 person-years), New Zealand (14.8 per 100,000 person-years), and the United States (14.8 per 100,000 person-years).
Among the 27 countries with increasing early-onset CRC rates, those with the steepest rises were observed in New Zealand with an average annual percentage change of 3.97% followed closely by Chile (3.96%) and Puerto Rico (3.81%). The other 23 countries showed stable incidence rates of early-onset disease.
In 14 of the 27 countries or territories including Australia, Canada, and the United States, the increase was exclusive to early-onset disease, whereas older adults showed stable or decreasing trends.
The sex-specific analysis revealed a faster increase among men in eight countries, including Chile and Puerto Rico, whereas six countries, including England and Norway, saw faster increases among women.
IN PRACTICE:
“The increase in early-onset colorectal cancer, previously seen predominately in high-income western countries, has now been documented in various economies and regions worldwide, marking it as a global phenomenon,” the study authors wrote. “The findings underscore the need for intensified efforts to identify factors driving these trends and increase awareness to help facilitate early detection.”
The authors added that “educational efforts to increase awareness of the increase in the incidence of early-onset colorectal cancer and its unique symptoms, especially among primary care providers, would have far reaching effects in reducing delayed diagnoses and mortality.”
SOURCE:
The study, led by Hyuna Sung, PhD, American Cancer Society in Atlanta, was published online in The Lancet Oncology.
LIMITATIONS:
According to the authors, the study was limited by underrepresentation of countries in Africa, Asia, and small islands where ongoing socioeconomic transitions might increase CRC rates.
DISCLOSURES:
This study received funding from the Intramural Research Program of the American Cancer Society, Cancer Grand Challenges, and National Institutes of Health. Additional disclosures are noted in the original article.
Lung cancer increasing among non-smokers, WHO warns
Being a non- or never-smoker appears to provide little protection against the ravages of cancer nowadays, with an increasing proportion of people being diagnosed with lung cancer who have never lit up, and with air pollution being an “important factor”, the World Health Organisation’s cancer agency has said.
Lung cancer in people who have never smoked cigarettes or tobacco is now estimated to be the fifth highest cause of cancer deaths worldwide, according to the International Agency for Research on Cancer (IARC).
In never-smokers, it is also occurring almost exclusively as adenocarcinoma, which has become the most dominant of the four main subtypes of the disease in both men and women globally.
About 200 000 cases of adenocarcinoma were associated with exposure to air pollution in 2022, according to the IARC study published in The Lancet Respiratory Medicine journal.
The largest burden of adenocarcinoma attributable to air pollution was found in east Asia, particularly China.
The study’s lead author and head of the IARC’s cancer surveillance branch, Dr Freddie Bray, toldThe Guardianthat the findings underscored the need for urgent monitoring of the changing risk of lung cancer.
Further studies were also required to identify possible causal factors, like air pollution, in populations where smoking was not considered the main cause of lung cancer, he added.
“With declines in smoking prevalence – as seen in the UK and US – the proportion of lung cancers diagnosed among those who have never smoked tends to increase,” Bray said. “Whether the global proportion of adenocarcinomas attributable to ambient air pollution will increase depends on the relative success of future strategies to curtail tobacco use and air pollution worldwide.”
Lung cancer remains the leading cause of cancer incidence and mortality worldwide. In 2022, about 2.5m people were diagnosed with the disease. But the patterns of incidence by subtype have changed dramatically in recent decades.
Of the four main subtypes of lung cancer (adenocarcinoma, squamous cell carcinoma, small-cell carcinoma and large-cell carcinoma), adenocarcinoma has become the dominant subtype among both men and women, the IARC found.
Adenocarcinoma accounted for 45.6% of global lung cancer cases among men and 59.7% of global lung cancer cases among women in 2022. The respective figures were 39.0% and 57.1% in 2020.
Adenocarcinoma accounts for as much as 70% of lung cancer cases among never-smokers, the IARC said.
While lung cancer incidence rates for men have generally decreased in most countries during the past 40 years, rates among women have tended to continue to rise.
Current trends suggest that while men still comprise most lung cancer cases (about 1.6m in 2022), the gap between lung cancer incidences in males and females is narrowing, with about 900 000 women diagnosed with lung cancer in 2022.
In 2023, The Guardian revealed how the number of women diagnosed with lung cancer in the UK was overtaking men for the first time, prompting calls for women to be as vigilant about it as they are about breast cancer.
Cancer experts said the figures reflected historical differences in smoking prevalence, specifically that smoking rates peaked much earlier in men than women. Women should now be as alert to potential lung cancer signs as they were about checking for lumps in their breasts, they said.
Changes in cigarette manufacturing and smoking patterns in recent decades have influenced the trends in lung cancer incidence by subtype, and there is accumulating evidence of a causal link between air pollution and an increased risk of adenocarcinoma, the IARC said.
It is not known what proportion of global lung cancer cases are in never-smokers, only that evidence suggests it is rising. Scientists are racing to learn more about what else is causing lung cancer, beyond smoking.
“Air pollution can be considered an important factor partly explaining the emerging predominance of adenocarcinoma that accounts for 53% to 70% of cases of lung cancer among people who have never smoked worldwide,” the study reported.
Bray said the research provided important insights into how both lung cancer and the underlying risk factors were evolving, “offering clues as to how we can optimally prevent lung cancer worldwide”.
“Changes in smoking patterns and exposure to air pollution are among the main determinants of the changing risk profile of lung cancer incidence by subtype that we see today.
“The diverging trends by sex … offer insights to cancer prevention specialists and policymakers seeking to develop and implement tobacco and air pollution control strategies tailored to high-risk populations.”
Study details
Estimated worldwide variation and trends in incidence of lung cancer by histological subtype in 2022 and over time: a population-based study
Ganfeng Luo, Yanting Zhang, Jerome Vignat et al.
Published in The Lancet Respiratory Journal on 3 February 2025
Summary
Background Lung cancer is the most common cancer worldwide, yet the current epidemiological profile of lung-cancer incidence by histological subtype is only partly understood. We aimed to assess geographical variation in incidence of lung cancer by subtype worldwide in 2022, geographical variation in adenocarcinoma incidence attributable to ambient particulate matter (PM) pollution worldwide in 2022, temporal trends in lung-cancer incidence by subtype from 1988 to 2017 in 19 countries, and generational changes.
Methods For this population-based study, we used data from the Global Cancer Observatory (GLOBOCAN) 2022, Cancer Incidence in Five Continents Volumes VII–XII, and members of the African Cancer Registry Network. To obtain national estimates of lung cancer in 2022 for the four main histological subtypes (ie, adenocarcinoma, squamous cell carcinoma [SCC], small-cell carcinoma, and large-cell carcinoma) by year, sex, and age group, we combined national estimates with representative, subsite-specific incidence proportions of lung cancer on the basis of recorded incidence data compiled in Cancer Incidence in Five Continents Volume XII and from members of the African Cancer Registry Network. We calculated country-specific, sex-specific, and age-specific proportions of and sex-specific and age-specific incidence rates per 100 000 people for all four histological subtypes. To account for differences in age composition between populations by country, we calculated age-standardised incidence rates (ASRs) per 100 000 people for lung cancer by subtype and sex at national and regional levels. We also quantified the burden of adenocarcinoma incidence attributable to ambient PM pollution for 179 countries in 2022. We conducted joinpoint regression and age-period-cohort analysis to assess temporal trends in ASRs in 19 countries by sex.
Findings In 2022, we estimated that there were 1 572 045 new cases of lung cancer worldwide among male individuals, of which 717 211 (45·6%) were adenocarcinoma, 461 171 (29·4%) were SCC, 180 063 (11·5%) were small-cell carcinoma, and 101 861 (6·5%) were large-cell carcinoma. In 2022, we estimated that there were 908 630 new cases of lung cancer worldwide among female individuals, of which 541 971 (59·7%) were adenocarcinoma, 155 598 (17·1%) were SCC, 87 902 (9·7%) were small-cell carcinoma, and 59 271 (6·5%) were large-cell carcinoma. Among male individuals, the highest ASRs were in east Asia for adenocarcinoma (27·12 [95% CI 27·04–27·21] per 100 000 people), east Europe for SCC (21·70 [21·51–21·89] per 100 000 people) and small-cell carcinoma (9·85 [9·72–9·98] per 100 000 people), and north Africa for large-cell carcinoma (4·33 [4·20–4·45] per 100 000 people). Among female individuals, the highest ASRs were in east Asia for adenocarcinoma (19·04 [18·97–19·11] per 100 000 people), north America for SCC (5·28 [5·21–5·35] per 100 000 people) and small-cell carcinoma (4·28 [4·21–4·35] per 100 000 people), and north Europe for large-cell carcinoma (2·87 [2·78–2·96] per 100 000 people). We estimated that 114 486 adenocarcinoma cases among male individuals and 80 378 adenocarcinoma cases among female individuals were attributable to ambient PM pollution worldwide in 2022, with ASRs of 2·35 (95% CI 2·33–2·36) per 100 000 male individuals and 1·46 (1·45–1·47) per 100 000 female individuals. Temporal trends in lung-cancer incidence by subtype and sex during 1988–2017 varied considerably across the 19 countries.
Interpretation Estimated geographical and temporal distribution of lung-cancer incidence varied across the four main subtypes worldwide. Our study highlights the need for future studies that identify possible causal factors that contribute to the changing risk patterns of lung cancer.
Using AI with mammography can help select women at high risk of breast cancer for supplemental MRI, according to research published February 4 in Radiology.
A team led by doctoral candidate Suzanne van Winkel from the Radboud University Medical Center in Nijmegen, the Netherlands, found that a commercially available AI system successfully identified high-risk women for breast MRI in an intermediate-risk study population, including women with occult cancers on mammography.
“AI selection of women with intermediate risk for supplemental MRI screening has the potential to reduce screening burden and costs while maintaining a high cancer detection rate,” the van Winkel team wrote.
Women at high risk of breast cancer, such as those with a personal history or family history of the disease or those with dense breasts, may be recommended for supplemental imaging. However, access to MRI can be limited for some women.
Van Winkel and colleagues suggested that selecting women for MRI by assessing their mammograms could make way for screening that effectively uses resources in breast imaging facilities and hospitals.
Using a retrospective dataset, they explored the feasibility of using an AI system (Transpara version 1.7.0, ScreenPoint Medical) for breast cancer detection on 2D mammograms to triage women with an assumed intermediate breast cancer risk for supplemental MRI. The team also investigated whether patient factors influenced the chance of a false-negative AI result. The AI system provided a case-based score that ranked the likelihood of malignancy on a scale of 1 to 10.
The study included data from 760 women with an average age of 48.9 years. From these women, the study also included data from 2,819 combined screening exams, from which 37 breast cancers were detected.
Images depict a 55-year-old woman with a family history of breast cancer who underwent combined mammography and MRI screening. (A) Right and (B) left mediolateral oblique and (C) right and (D) left craniocaudal mammograms show a large known cyst in the left breast (arrow in B and D), but were otherwise assessed as being unremarkable. Breast tissue was judged to be extremely dense. (E) Concurrent axial subtraction MRI scan shows a large, diffuse, invasive lobular cancer (circle) in the right breast. The AI system provided a case-based cancer suspicion score of 8 on a scale of 0-10, which would have led to selection for MRI screening using both the score 5 and score 8 thresholds, but not the score 9 threshold.RSNA
Using AI at mammography achieved an area under the receiver operating characteristic curve (AUROC) of 0.72 for the entire intermediate-risk population and an AUROC of 0.81 for women with prior breast cancer.
The researchers also analyzed breast cancers detected by AI for different recall thresholds. An AI score of five indicated about 50% of women recalled, a score of 8 indicated about 20% of women recalled, and a score of 9 indicated about 10% of women recalled.
Using a threshold score of 5, 31 of the total breast cancers (84%) were detected, including 13 of 19 (68%) mammographically occult cancers, for a supplemental breast MRI rate of 50% (1,409 of 2,819 exams).
Finally, the team observed no significant association between breast density or age and the probability of a false-negative AI result.
The study authors highlighted that using AI in this manner could improve screening results while also reducing unnecessary costs.
“The use of AI might also reassure patients in cases where the radiologist and AI results agree that screening results are negative, which could potentially reduce the demand for breast MRI,” they concluded.
Lung Cancer Screening Is the Push Smokers Need to Quit
Nadine Eckert
February 07, 2025
Quitting smoking is challenging, particularly when resources are limited. A recent study in the United States confirmed that an intensive program combining behavioral therapy and medication, linked to a lung cancer screening program, offers the highest success rate. However, its long-term success was similar to that of telephone counselling and drug therapy.
Pulmonologist and experienced smoking cessation specialist from Stuttgart, Germany, Alexander Rupp, MD, emphasized the importance of leveraging routine healthcare interactions to encourage smoking cessation. “Although every doctor-patient contact offers the opportunity to discuss the risks of smoking and the opportunities for smoking cessation, the ‘window of opportunity’ is very wide, especially during lung cancer screening,” he said.
Germany is preparing to launch a lung cancer screening program for high-risk individuals, primarily current smokers and former smokers. Following the establishment of radiation protection regulations for such a program last year, the German Federal Joint Committee is currently working on its design. The initiative could be a game-changer for smoking cessation.
Lung cancer screening has been available for smokers in the United States for some time. Paul M. Cinciripini, PhD, and colleagues from the University of Texas MD Anderson Cancer Center, Houston, examined three smoking cessation strategies with decreasing treatment intensity among screening participants.
Unique Opportunity
Previous studies have shown that participation in a lung cancer screening program — typically offered only to high-risk individuals — significantly increases motivation to quit smoking.
“Repeated contact with doctors, repeated CT scans, and especially the findings that require monitoring all contribute to this effect.” explained Rupp, who regularly offers smoking cessation courses.
It has long been known how smoking cessation works best. “The gold standard is a combination of behavioral therapy support and drug treatment — if there is an addiction and withdrawal symptoms occur after quitting, which is the case for the majority of smokers,” Rupp explained.
The US study reinforced what is already well known: More intensive treatment approaches lead to higher quit rates.
“We know that the more intensively we look after smokers, the higher the quit rate. This applies in both areas: The more therapy sessions we do and the more often we prescribe medication, the more likely the patients are to succeed in remaining abstinent,” Rupp said.
However, resources for intensive smoking cessation programs are limited. A database maintained by the German Cancer Research Center and the German Federal Center for Health Education lists only 455 providers of smoking cessation courses in Germany, “not all of which even work on an evidence-based basis,” Rupp emphasized. Given that there are around 16 million smokers in Germany, there is an urgent need for smoking cessation programs that are less resource-intensive.
Intensity Variations
The US study compared three smoking cessation strategies of varying intensities, integrating behavioral counseling and medication.
Group 1: An integrated program with eight behavioral therapy sessions and 10-12 weeks of nicotine replacement therapy or medication (bupropion or varenicline).
Group 2: Lighter version of the integrated program. It consisted of four telephone consultations, written materials, online support, and 12 weeks of nicotine replacement therapy or medication prescribed by a radiologist.
Group 3: The least intensive approach, with 12 weeks of nicotine replacement therapy alone.
Each strategy was evaluated in 210 lung cancer screening participants aged 55-64 years who smoked an average of 15-20 cigarettes per day.
After 3 months, significantly more participants in the most intensive program (Group 1, 37.1%) had quit smoking than those in the other two groups (Group 2, 27.1%; Group 3, 25.2%).
But after 6 months, the difference between Groups 1 and 2 was not significant. The quit rates were as follows: Group 1, 32.4%; Group 2, 27.6%; and Group 3, 20.5%.
“It can be concluded from these results that the intensity of smoking cessation can be reduced to a certain extent as long as the combination of behavioral counseling and medication is given,” Rupp concluded.
Digital Solutions
Another new possibility, which was not examined in the US study, is digital health applications.
Smoke Free is a digital health application that provides behavioral therapy support for smoking cessation and is available in both German and English. Designed to replicate structured smoking cessation programs and offers an accessible alternative for individuals seeking to quit smoking.
Rupp emphasized the potential of digital tools like Smoke Free to expand access to effective smoking cessation strategies, particularly for those unable to attend in-person programs. While traditional cessation programs are limited in availability, digital apps can increase engagement in and adherence to smoking cessation efforts.
However, the biggest hurdle is smokers’ procrastination: “If you make smokers an offer, they usually do not take action afterward because they are caught in their ambivalence about whether they should quit or not.”
Policy Implications
This makes smoking cessation a mandatory component of lung cancer screening in the future. “It’s about cancer, and patients are really afraid of that,” Rupp advocated.
In a position paper, the German Respiratory Society, supported by multiple medical societies, has called for smoking cessation to be integrated into lung cancer screening protocols, with full coverage of counseling and medication by health insurance.
“Smoking cessation must be a mandatory component. If a participant in the lung cancer screening does not want this, then he or she must actively object,” stressed Rupp, lead author of the position paper. Also, the costs of smoking cessation, including those of withdrawal-inhibiting medication, must be fully covered by statutory health insurance, which has not been the case to date.
“That’s the only thing that makes sense. You can’t deny an addict access to proven treatments, especially when we know that a smoker who quits spontaneously without support has a relapse rate of 95%-97%, and the medication per se increases the quit rate by a factor of 2 or 3,” Rupp concluded.
This story was translated and adapted fromMedscape’s German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Lung cancer screening with low-dose CT can detect extensive coronary artery calcium (CAC), an independent predictor of all-cause death and cardiovascular events, new research suggests.
Gary Small, MBChB, PhD
“The high prevalence of asymptomatic coronary artery disease (83%) was surprising, as was the prevalence of extensive CAC (30%),” principal investigator Gary Small, MBChB, PhD, a cardiologist at the University of Ottawa Heart Institute, Ottawa, Ontario, Canada, told Medscape Medical News.
“The size of effect was also surprising, as was the persistence of the effect even in the presence of elevated mortality risk from other causes,” he said. “Extensive coronary disease was associated with a twofold increase in risk for death or cardiovascular events over 4 years of follow-up,” even after adjustment for risk for death from cancer and other comorbidities such as chronic obstructive pulmonary disease.
“CAC as reported on chest CT exams is often ignored and not factored into clinical practice,” he noted. “The presence of CAC, however, provides a very real and very personal perspective on an individual’s cardiovascular risk. It is a true example of personalized medicine.”
The study was published online on December 2 in the Canadian Medical Association Journal.
Air Pollution Exposure Linked to Higher Breast Cancer Risk
Edited by Gargi Mukherjee
October 24, 2024
TOPLINE:
A recent study found that long-term exposure to fine particulate matter ≤ 2.5 μm (PM2.5) is associated with an increased risk for breast cancer, with the highest risk observed among White women.
METHODOLOGY:
Studies have suggested that exposure to air pollution — specifically PM2.5 — may increase the risk for breast cancer, but data are largely in populations of White women.
The current analysis explored the potential risk among a more racially and ethnically diverse group.
The study included 58,358 women (median age, 60.4 years at enrollment) from the California Cancer Registry, followed over an average of 19.3 years. Overall, 35% were African American, 39% were Latino, 15% were White, and 10% were Japanese American.
Researchers measured PM2.5 exposure using satellite-based data and geocoded addresses. Other pollutants, such as PM10, NO2, NOX, and CO, were also tracked using Environmental Protection Agency data.
TAKEAWAY:
A total of 3524 invasive breast cancer cases were diagnosed over an average follow-up period of 19.3 years. PM2.5 exposure was associated with a 28% increased risk for breast cancer overall (hazard ratio [HR], 1.28; 95% CI, 1.08-1.51).
When looking at risk by racial/ethnic group, the association between PM2.5 exposure and breast cancer risk was strongest among White women (HR, 1.67). PM2.5 exposure was also associated with a higher risk for breast cancer among African American women (HR, 1.14; 95% CI, 0.89-1.46) and Latino women (HR, 1.34; 95% CI, 0.94-1.92), but the associations were not significant.
Overall breast cancer incidence was also positively associated with exposure to NO2, NOX, and CO (HRs, 1.09-1.11), but the associations were not significant. A meta-analysis of this study and ten other cohorts estimated a 5% increased breast cancer incidence per 10-unit increase in PM2.5 (HR, 1.05).
IN PRACTICE:
“Collective findings suggest that PM2.5 exposure should be considered a risk factor for breast cancer, and curtailing air pollution exposures at the population level using regulatory strategies should be a priority,” the authors concluded.
SOURCE:
The study, led by Anna H. Wu, PhD, MPH, Keck School of Medicine, University of Southern California, Los Angeles, was published online in the Journal of Clinical Oncology.
LIMITATIONS:
The study did not include data on nonresidential exposures or residential history before cohort entry, which limited the assessment of earlier exposures. The study also lacked information on specific sources of PM emissions, as well as an explanation for why White women had the highest breast cancer risk compared with other racial/ethnic groups.
DISCLOSURES:
The study was supported by grants from the Health Effects Air Pollution Foundation, the National Cancer Institute, USC Environmental Exposures, Host Factors, and Human Disease, and the California Air Resource Board. One author disclosed being an associate editor for the Journal of Clinical Oncology. No other potential conflicts of interest were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
The American College of Obstetricians and Gynecologists (ACOG) has updated its breast cancer screening guidelines, recommending that individuals at an average risk for breast cancer initiate mammography screening at age 40. This change reflects evolving evidence that starting earlier screening yields greater net benefits in reducing breast cancer mortality, particularly for certain racial groups with higher risk factors.
Breast cancer is the second leading cause of cancer deaths in American women overall and the leading cause of cancer deaths among Black and Hispanic women. Although mammography has long been recognized as a life-saving tool by detecting cancer early, there has been debate on when screening should begin due to concerns about overdiagnosis, false positives, and potential harms such as unnecessary biopsies.
Recent evidence has prompted ACOG to revise its recommendation for individuals assigned female at birth, including cisgender women, transgender men, and nonbinary individuals. This updated guidance includes individuals with dense breast tissue or a family history of breast cancer but excludes those with higher risk factors, such as a personal history of breast cancer or previous high-risk lesion on a breast biopsy, genetic mutations linked to higher cancer risk, or a history of high-dose radiation therapy to their chest at a young age.
Under the new guidelines, routine screening mammography should start at age 40 and can be performed annually or every 2 years, based on an informed, shared decision-making process that considers the benefits and potential harms of frequent screening.
Previously, ACOG recommended initiating screening between ages 40 and 50, depending on individual risk factors and preferences, with screening required by age 50 at the latest. However, several factors, including an increasing incidence of breast cancer in younger women, have influenced the decision to lower the recommended starting age.
Increasing Incidence Among Younger Women
Between 2015 and 2019, the incidence of invasive breast cancer in women aged 40-49 years increased by approximately 2% per year.
“There has been a concerning trend of increasing breast cancer diagnoses among women in their 40s, and new data shows that earlier screening could make a significant difference in decreasing breast cancer deaths,” said Eve Zaritsky, MD, FACOG, co-author of the clinical practice update. “While screening can sometimes cause anxiety for people and even unnecessary follow-up, the benefits of diagnosing breast cancer earlier outweigh those risks enough to warrant starting to get mammograms at age 40.”
Studies commissioned by the US Preventive Services Task Force (USPSTF) show that starting mammography at age 40 provides a greater overall benefit than beginning at age 50. Early screening reduces the number of breast cancer deaths and increases life years gained when weighed against the harms of false positives, overdiagnosis, and benign biopsies.
Addressing Health Inequities
The benefits of earlier screening are expected to be particularly significant for Black women, who have disproportionately high mortality rates from breast cancer. Even though Black women have a lower overall incidence of breast cancer than White women, they have a 40% higher 5-year age-adjusted mortality rate from the disease and a 45% increased incidence of invasive breast cancer before age 50. Black women are also more likely to be diagnosed with aggressive subtypes, such as triple-negative breast cancer, which is harder to detect and treat and occurs at younger ages.
Racial disparities in breast cancer outcomes are deeply rooted in inequities in social determinants of health, such as access to care, housing, and environmental conditions. Black women are also less likely to receive timely or comprehensive treatment than White women, which contributes to worse survival rates even after adjusting for socioeconomic factors and insurance status.
“Our updated recommendation addresses important inequities in breast cancer diagnosis, treatment, and death, and we hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” added co-author Cherie C. Hill, MD, FACOG.
ACOG’s updated recommendation aligns with that of other leading organizations, including the USPSTF, the National Comprehensive Cancer Network, the American College of Radiology, and the Society of Breast Imaging. This growing consensus among experts is expected to reduce confusion among clinicians and patients regarding when to begin screening, thus improving screening rates in individuals in the 40- to 49-year age group.
Zaritsky and Hill reported no conflicts of interest.
Meg Barbor is a freelance writer for Medscape Medical News.
Losses of muscle and strength are inescapable effects of the aging process. Left unchecked, these progressive losses will start to impair physical function.
Once a certain level of impairment occurs, an individual can be diagnosed with sarcopenia, which comes from the Greek words “sarco” (flesh) and “penia” (poverty). Individuals with sarcopenia have a significant increase in the risk for falls and death, as well as diminished quality of life.
Muscle mass losses generally occur with weight loss, and the increasing use of glucagon-like peptide-1 (GLP-1) medications may lead to greater incidence and prevalence of sarcopenia in the years to come.
A recent meta-analysis of 56 studies (mean participant age, 50 years) found a twofold greater risk for mortality in those with sarcopenia vs those without. Despite its health consequences, sarcopenia tends to be underdiagnosed and, consequently, undertreated at a population and individual level. Part of the reason probably stems from the lack of health insurance reimbursement for individual clinicians and hospital systems to perform sarcopenia screening assessments.
In aging and obesity, it appears justified to include and emphasize a recommendation for sarcopenia screening in medical society guidelines; however, individual patients and clinicians do not need to wait for updated guidelines to implement sarcopenia screening, treatment, and prevention strategies in their own lives and/or clinical practice.
Simple Prevention and Treatment Strategy
Much can be done to help prevent sarcopenia. The primary strategy, unsurprisingly, is engaging in frequent strength training. But that doesn’t mean hours in the gym every week.
With just one session per week over 10 weeks, lean body mass (LBM), a common proxy for muscle mass, increased by 0.33 kg, according to a study which evaluated LBM improvements across different strength training frequencies. Adding a second weekly session was significantly better. In the twice-weekly group, LBM increased by 1.4 kg over 10 weeks, resulting in an increase in LBM more than four times greater than the once-a-week group. (There was no greater improvement in LBM by adding a third weekly session vs two weekly sessions.)
Although that particular study didn’t identify greater benefit at 3x/week compared with 2x/week, the specific training routines and lack of a protein consumption assessment may have played a role in that finding.
Underlying the diminishing benefits, a different study found a marginally greater benefit in favor of performing ≥ 5 sets per major muscle group per week compared with < 5 sets per week for increasing muscle in the legs, arms, back, chest, and shoulders.
Expensive gym memberships and fancy equipment are not necessary. While the use of strength training machines and free weights have been viewed by many as the optimal approach, a recent systematic review and meta-analysis found that comparable improvements to strength can be achieved with workouts using resistance bands. For those who struggle to find the time to go to a gym, or for whom gym fees are not financially affordable, resistance bands are a cheaper and more convenient alternative.
A previous commentary outlined an overall approach to preventing loss of muscle mass while taking GLP-1–related medications. Of note, a diet with sufficient protein is critical for optimizing muscle mass gains as part of regular strength-training routines. One study performed in older adults with frailty found an average loss of 0.25 kg of LBM with consumption of 1.0 grams of protein per kilogram of total body weight per day (g/kg/d) despite 2 days of strength training per week for 24 weeks. In that same study, consuming 1.3 g/kg/d of protein led to an average increase of 1.25 kg of LBM during the same period and in association with the same strength-training routine as those consuming 1.0 g/kg/d. Meta-analyses performed to assess an amount of protein to provide optimal benefit to strength and muscle for strength-training individuals determined those amounts to be 1.5 g/kg/d and 1.62 g/kg/d, respectively. While historically a low-protein diet was recommended to prevent disease progression in individuals with chronic kidney disease(CKD), a recent study found reduced risk for death in patients with CKD with greater reported protein consumption. A separate study, using a mendelian randomization methodology, found a similar reduction in mortality risk among individuals with CKD who consumed greater amounts of protein.
Patients in Need of Sarcopenia Assessments
Although a gradual loss of muscle mass occurs over the course of life, sharp declines can also occur following an illness or an injury involving long bedrest. For example, one studyfound that 5 days of limb immobilization led to a 1.5% loss of quadriceps volume, equivalent to an amount of muscle loss, that, when extrapolated to the full body, may require 10 weeks of strength training twice weekly to regain.
In weight loss, such as from GLP-1–related medications, the sarcopenia risk may accrue long term, as it does in aging. Individuals who lose weight using GLP-1s may experienceimproved physical function in the short term (a little over a year), despite 20%-40% of the total weight lost coming from muscle mass; however, this loss of muscle may cause limitations over time.
If someone lost 20 lb of their total body weight through the use of semaglutide and was not strength training and not consuming enough protein, the amount of LBM lost (assuming 40% of total weight lost) is 8 lb or 3.62 kg. If a body-composition assessment was not performed before and after the weight loss, it won’t be possible to estimate how much of the lost weight is coming from muscle compared with fat. This individual may not yet experience a loss in strength as a result of that muscle loss, particularly if they are in their 50s; however, a person in their 70s is more likely to experience some degree of limitation in their physical function as a result.
For some individuals, that amount of muscle mass reduction can tip them into the sarcopenic range, which increases the risk for hip fractures. Sarcopenia contributed to 71% of hip fractures in one community-level study. Hip fractures are not uncommon. One studyreported a lifetime risk for a hip fracture of 16%-18% in White women of and 5%-6% in White men. Furthermore, 34% of older adult patients who suffer a hip fracture die within 1 year of the fracture, and of those who survive, many experience impaired mobility and quality of life even up to 2 years afterward.
To outline an unfortunate but possible trajectory, an individual could unknowingly lose muscle in association with weight loss achieved in their 50s, acquire a mild case of pneumonia at a social event in their 60s or 70s, end up in the hospital for 7 days undergoing treatment for pneumonia, experience a rapid loss of muscle mass during the hospitalization, leave the hospital after completing pneumonia treatment, only to then fall ascending the stairs to their home, suffer a hip fracture, and end up back in the hospital.
How Do Busy Clinicians Fit In Sarcopenia Screening?
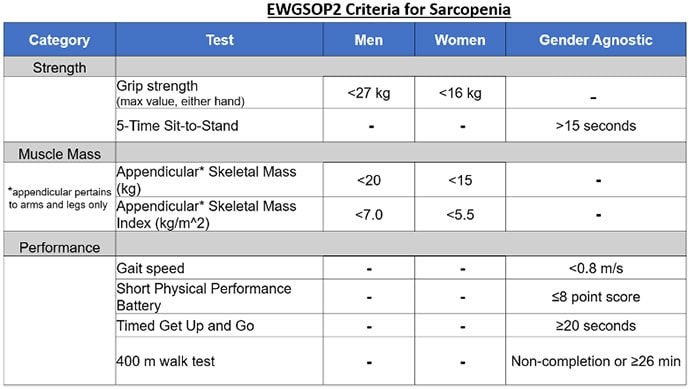
Different sarcopenia-related societies have proposed different criteria and thresholds for diagnosis. Of these different guidelines, those from the European Working Group on Sarcopenia in Older People (EWGSOP) are the most recent and are summarized below:
EWGSOP-defined sarcopenia categories:
One criterion met = Probable sarcopenia
Two criteria met = Sarcopenia
Three or more criteria met = Severe sarcopenia
An assessment for sarcopenia does not require excessive time, cost, or safety risk. Of the tests included for screening for sarcopenia in the EWGSOP criteria, grip strength and the 5-Time Sit-to-Stand (5tStSt) assessments are probably the most feasible to perform in clinic. These are evidence-based and can be performed together in about 2 minutes total time.
Hand Grip Strength
The clinically validated Jamar Hydraulic Hand Dynamometer is available for about $270, but devices priced at $30 are probably reasonably accurate and worthy of consideration for clinics with budgetary limitations. To perform the grip strength test, the patient simply squeezes the device with as much force as they can, once with each hand. The device will display the max force generated with each squeeze.
5-Time Sit Stand to Test
For the 5tStSt, the patient should begin in a seated position, cross their arms over their shoulders (so that their hands are not used to assist in the movement), and rise to a full stand before returning to a seated position. This motion should be completed five times, and the patient should be instructed to complete the five repetitions as quickly as possible, while the time required to complete the five repetitions is recorded.
Ideally, if performed during a clinic visit, the clinicians would show the patient how their results compare with demographic norms for each test; see here for examples of demographic norms for grip strength and here for the 5tStSt.
Body Composition Assessments
Body composition data are also included as part of a sarcopenia assessment and have gender-specific thresholds defined in the EWGSOP criteria. A body composition assessment provides data on LBM (which is a proxy for muscle mass) and fat mass. A recent study demonstrated that percent body fat provides greater sensitivity than body mass index for diagnosing obesity and metabolic syndrome.
When to Consider Sarcopenia Screening
An extensive body of evidence on sarcopenia supports sarcopenia screening for all patients older than age 65. Given the risk for muscle mass reductions that occur with weight loss in general and GLP-1–related medications more specifically, sarcopenia screening is probably appropriate for certain patients younger than 65 years as well.
Clinical judgement should be used to determine when and whom to assess for sarcopenia; however, given that the screening assessments are fast, safe, and have minimal cost, a low threshold for screening appears appropriate. For example, even for a 50-year-old patient who has not been physically active, sarcopenia assessments may indicate below-average performances, and this knowledge can serve as motivation for this patient to adopt an exercise regimen to address strength-related limitations that have already begun to manifest. Further, keeping a record of screenings performed in younger years can serve as points of comparison for repeat assessments later on.
Self-Directed Sarcopenia Screening
Some healthcare providers may not be familiar with the diagnostic criteria for sarcopenia; efforts to promote greater awareness and testing should continue. That said, patients can perform some of the testing themselves if so desired.
The 5tStSt, 400-meter walk test, and Timed Get Up and Go (TUG) tests do not require a clinician. The 400-meter walk test simply evaluates the time required for completion of walking this distance. The TUG test evaluates the time required for a patient to rise from a chair and then walk 3 meters forward. As part of the TUG test, patients can use their arms to assist in rising from the chair.
It has been said that every job has a “sales” component. This is also true of medicine. Doctors must “sell” patients on an explanation for their symptoms and must elicit “buy-in” from them on a treatment plan for it to be most effective. Data from sarcopenia assessments can increase the power of the sales pitch aimed at motivating patients to adopt and/or improve an exercise routine.