
Use D-dimer, CTPA to gauge PE risk in COVID-19 patients
By Kate Madden Yee, AuntMinnie.com staff writer
Patients with COVID-19 who have high D-dimer levels are good candidates for CT pulmonary angiography (CTPA) to rule out acute pulmonary embolism (PE), according to a study published June 9 in European Radiology.
The findings suggest a way clinicians can better evaluate the embolism risk in patients, since disease severity isn’t necessarily a significant measure, wrote a team led by Dr. Alban Gervaise of Military Hospital Begin in Saint-Mandé, France.
In fact, Gervaise and colleagues found that almost 20% of nonhospitalized patients with COVID-19 referred to CTPA by emergency department staff had acute pulmonary embolism — underscoring the importance of not making assumptions about patients with COVID-19 by the presenting acuity of the disease.
“Severity and radiological features of COVID-19 pneumonia showed no significant difference between patients with or without acute pulmonary embolism,” the team wrote.
Avoid assumptions
Noncontrast chest CT — in conjunction with reverse transcription polymerase chain reaction (RT-PCR) testing — has been shown to be a useful tool for evaluating the pulmonary involvement of COVID-19, the authors wrote. CTPA’s use has been more limited, mostly in patients whose condition has worsened and in whom doctors want to check for acute pulmonary embolism.
Studies have confirmed a link between COVID-19 and acute pulmonary embolism in hospitalized patients with severe to critical illness, but it’s important not to assume that embolism is only present in this population, according to Gervaise and colleagues.
“In our practice, we have found cases of acute pulmonary embolism in nonhospitalized COVID-19 patients referred to CTPA by our emergency department,” they wrote.
The researchers sought to investigate the prevalence of acute pulmonary embolism in patients referred to CTPA by the emergency department. They conducted a retrospective study that included 72 patients who underwent CTPA between March 14 and April 6. Two radiologists evaluated the patients’ scans for acute pulmonary embolism; Gervaise’s team compared the clinical classification (minimal, moderate, severe, critical), lung involvement, and CT total severity score of patients with embolism and those without.
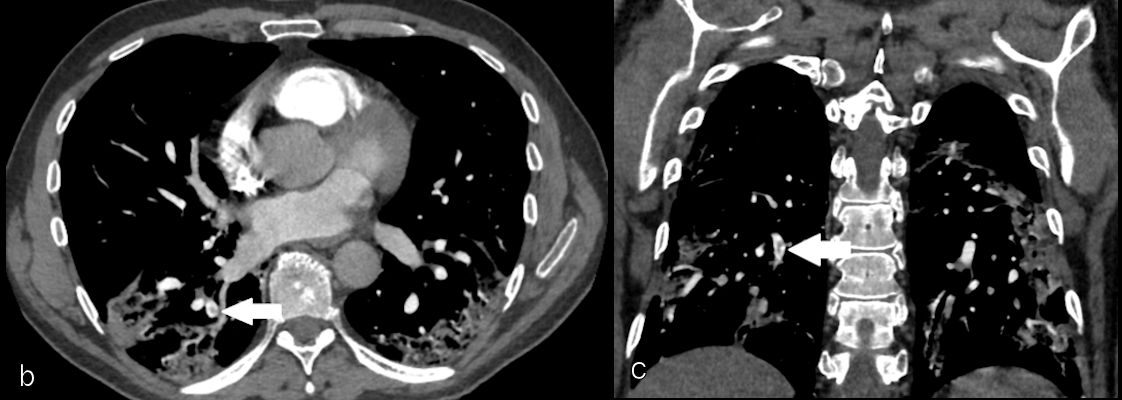
Of the 72 patients who underwent CTPA, 80% also had a positive RT-PCR test for SARS-CoV-2. CTPA identified embolism on 13 scans (18%). Of these, two had main, four had lobar, and seven had segmental acute pulmonary embolism. The most commonly affected lung segments were right lower lobe (61%) and left lower lobe (54%).
The investigators found that mean age and D-dimer values were higher in patients with embolism compared with those without, but they didn’t find a statistically significant difference between the two groups when it came to clinical type, lung lesions, CT severity scores, quality of the CTPA exam, or pleural effusion.
| CTPA results in patients with and without acute pulmonary embolism | |||
| Characteristic | Patients with acute pulmonary embolism | Patients without acute pulmonary embolism | P-value |
| Mean age | 74 | 60 | 0.008 |
| D-dimer | 7.29 µg/ml | 3.29 µg/ml | 0.011 |
| Radiological findings | |||
| Ground-glass opacity | 85% | 97% | 0.147 |
| Consolidation | 69% | 68% | 1 |
| Crazy paving | 38% | 37% | 1 |
| Linear reticulation | 69% | 78% | 0.490 |
| CT severity score | 6.3 | 7.1 | 0.365 |
| Quality of CTPA exam | 1.8 | 2 | 0.518 |
| Pleural effusion | 38% | 19% | 0.146 |
“Thirteen acute pulmonary embolisms were discovered [with CTPA], representing a prevalence of 18% of the patients included in our study,” the team noted. “Eight patients with acute pulmonary embolism had a severe to critical COVID-19 pneumonia but five of the 13 (38%) patients with acute pulmonary embolism had moderate clinical form. These results seem to confirm the association between COVID-19 and acute pulmonary embolism, even in nonsevere and nonhospitalized COVID-19 patients.”

 .
.
Valuable measure
The D-dimer level of a patient seems to be a valuable data point for assessing the severity of COVID-19 and the possibility of acute pulmonary embolism — and therefore the need for CTPA for further workup, according to the authors.
“Given that the increase in D-dimer level can be linked to COVID-19, it would be interesting to evaluate … if there is a cutoff D-dimer level at which CTPA could be recommended to search for acute pulmonary embolism in COVID-19 patients,” the team concluded. “Pending further data on D-dimer levels, we believe that all patients with COVID-19 pneumonia and an increased level of D-dimer should benefit from CTPA to eliminate acute pulmonary embolism, whenever possible.”